







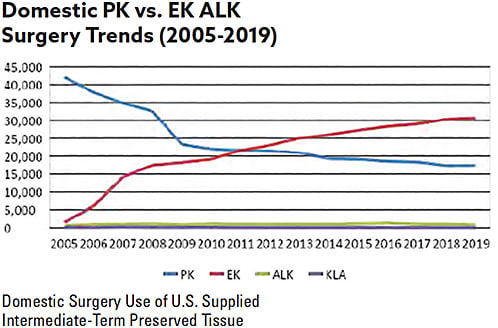
Since 2007, there has been a steady increase in the percentage of endothelial corneal transplants performed in the U.S. and elsewhere. In fact, in 2011, EK surpassed PK grafts in the U.S. and, 64% of corneal transplants were endothelial grafts.1 (See infographics below.)
| DOMESTIC SURGERY USE | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 |
| Total Endothelial Keratoplasty Procedures | 24,987 | 25,965 | 27,208 | 28,327 | 28,991 | 30,336 | 30,650 |
| DSEK, DSAEK, DLEK Procedures | 23,465 | 23,100 | 22,514 | 21,868 | 21,337 | 19,526 | 17,428 |
| DMEK or DMAEK Procedures | 1,522 | 2,865 | 4,694 | 6,459 | 7,628 | 10,773 | 13,215 |
| PDEK | 21 | 26 | 6 | ||||
| Other EK | 7 | 11 | 1 | ||||
| 2019 Eye Banking Statistical Report. Eye Bank Association of America. Washington, DC: April 13, 2020. | |||||||
Reasons for Increase
The reasons for the steady increase are related to the availability of pre-cut tissue and improved insertion devices.
In 2007, pre-cut Descemet’s stripping automated endothelial keratoplasty (DSAEK) tissue started to become more widely available and distributed by U.S. eye banks. This meant that surgeons no longer had to manually prepare Descemet’s stripping endothelial keratoplasty (DSEK) tissue or purchase expensive equipment to cut their own DSAEK tissue and risk tissue wastage.
As more eye banks began to offer this service, more surgeons transitioned to performing the DSAEK procedure by ordering pre-cut tissue, and the number of DSAEK transplants began to increase significantly.
New Methods
Today, surgeons can order varying thicknesses of DSAEK pre-cut tissue and also have a choice in DSAEK insertion devices. The EndoGlide (Network Medical, UK distributed in U.S. by Keramed Inc.) and EndoSerter (CorneaGen) both offer similar outcomes for DSAEK insertion and graft survival.2 Other options include Busin glide for a pull-through technique, 30 g needle for a push-in technique, with or without a Sheets glide, and DSAEK forceps. The variety of DSAEK insertion devices allows for surgeons to become proficient in a variety of techniques, depending on their preference, case and budget.
Additionally, there is the ability to custom order the preferred thickness of DSAEK grafts from eye banks, according to surgeon preferences. This allows for those surgeons interested in ultrathin DSAEK grafts to have those pre-prepared for utilization.
Similar to the greater adoption of DSAEK techniques that resulted from the availability of pre-cut DSAEK tissue, the availability of customized pre-cut DMEK tissue has placed DMEK at the forefront of growth in endothelial transplantation. Again, 64% of all corneal transplants in the U.S. were EK, with a 23% increase in DMEK.1
Preparing DMEK tissue is time consuming, adding significant time to an operating room case. Pre-stripped and pre-marked DMEK tissue was first made available around 2015, requiring surgeons to separate the pre-stripped tissue from the cap, and load into their insertion device of choice. These devices are the Geuder Glass Cannula (CorneaGen), the Melles Injector (DORC International) or the Straiko Modified Jones Tube (Gunther Weiss Scientific). Having pre-marked tissue has greatly improved the facility of the DMEK procedure, providing the surgeon with an easy way to identify the orientation of the tissue for proper unfolding.
Pre-cut and pre-loaded DMEK tissue, now widely available in the U.S. has also cut down on the time to prepare DMEK tissue. There are several options available. One can order pre-cut tissue to size and load it into their desired insertion device. This provides the ease of not having to strip the tissue, but rather simply remove it from the storage solution vial and load into the cannula, tube or IOL inserter.
Additionally, surgeons can order pre-loaded, pre-stripped and marked tissue. This improves operating room efficiency by having the prepared, pre-marked DMEK scroll “ready to go.” Pre-loaded tissue is available in a Geuder Glass Cannula (CorneaGen) and in a Straiko Modified Jones Tube (Gunther Weiss Scientific), both allowing for a small incision and requiring the attachment of a syringe for insertion.
A Win-Win
The innovations in DMEK tissue preparation have helped to increase adoption of the DMEK technique, which is shown to provide for faster and improved visual recovery, decreased higher-order aberrations, and better outcomes versus DSAEK.3,4 Innovations and improvements in EK tissue preparation allow today’s cornea surgeons to perform the procedures more efficiently and choose the type and preparation of tissue that can best suit their patients’ needs. CP
References:
- Eye Bank Association of America. 2019 Medical Standards. Washington, DC: Eye Bank Association of America; 2019.
- Elbaz U, Yeung SN, Lichtinger A, et al. EndoGlide versus EndoSerter for the insertion of donor graft in Descemet stripping automated endothelial keratoplasty. Am J Ophthalmol. 2014;158(2):257-262
- Price MO, Giebel AW, Fairchild KM, Price FW Jr. Descemet’s membrane endothelial keratoplasty: prospective multicenter study of visual and refractive outcomes and endothelial survival. Ophthalmology. 2009;116(12):2361-2368.
- Duggan M, Rose-Nussbaumer J, Lin CC, Austin A, Labadzinski PC, Chamberlain WD. Corneal higher-order aberrations in Descemet membrane endothelial keratoplasty versus ultrathin DSAEK in the Descemet endothelial thickness comparison trial: a randomized clinical trial. Ophthalmology. 2019;126(7):946-957.
