







Corneal opacification is a major cause of vision impairment and blindness worldwide.1 Most cases of corneal blindness can be successfully managed by performing a corneal transplantation.2 In fact, corneal transplantation or keratoplasty is the most commonly performed and successful form of organ or tissue transplantation in the history of medicine. However, there are a small group of conditions where corneal grafts have repeatedly failed or are very likely to fail if a keratoplasty is performed.3 This is because corneal transplants are allografts and carry the risk of immunological rejection, apart from failure due to surface- or suture-related complications. Typically, this risk is highest in corneal diseases with an underlying immunological or inflammatory etiology. It is in this select group of cases that a keratoprosthesis or KPro is indicated.3
A look at the Boston KPro
A KPro is an artificial corneal device that is implanted to restore vision in eyes with corneal blindness caused by conditions that are not amenable to even corneal transplantation.3 There are numerous different types of KPros that have been described in literature. The design that is most commonly performed worldwide is the Boston type 1 KPro (Boston Keratoprosthesis, a not-for-profit entity within Massachusetts Eye and Ear).4 However, even this device has limited retention in certain extreme cases which have ocular surface damage, particularly those with a dry or dermalized ocular surface.5,6 In these eyes with end-stage corneal or ocular surface disease, there are very few options, limited to the Boston type 2 and the osteo-odonto keratoprosthesis (OOKP).7,8 The OOKP requires a multidisciplinary and complex approach but has good long-term retention, among the longest reported for KPros.8 The main disadvantages are the requirement of dentulous patients and multiple stages until vision restoration. The Boston type 2 is, on the other hand, limited by its availability and cost.7 A third alternative in these extreme cases is an LVP KPro, which is based on the Boston KPro platform but is exposed through a mucous membrane graft or conjunctival flap instead of the eyelid.9
The Advantages of the LVP KPro
The advantages of the LVP KPro over the Boston type 2 KPro are that the eyelids are spared allowing the patients to blink or close their eyes, which is impossible with the type 2 design.10 It also allows topical medications to be instilled as the inferior fornix is intact, unlike the Boston type 2 where administering any topical medications is difficult and requires either oral administration or peribulbar injections for the management of any intraocular inflammation.9,10 Most centers that perform Boston type 2 KPros also combine it with a complete pars plana vitrectomy and glaucoma tube shunt procedure, because managing posterior segment complications or performing glaucoma surgeries require opening up of the eyelids. With the LVP KPros, these procedures can be performed in the usual way by either making ports through the mucosa or lifting the mucosal flap.9
Surgical Technique and Postoperative Care
The LVP KPro’s design and the associated surgical technique was first described in 2014.10 It is a modification of the Boston type 1 KPro design with an optical stem that is 0.75 mm longer. Unlike the Boston type 2 KPro it does not have an extra flange.
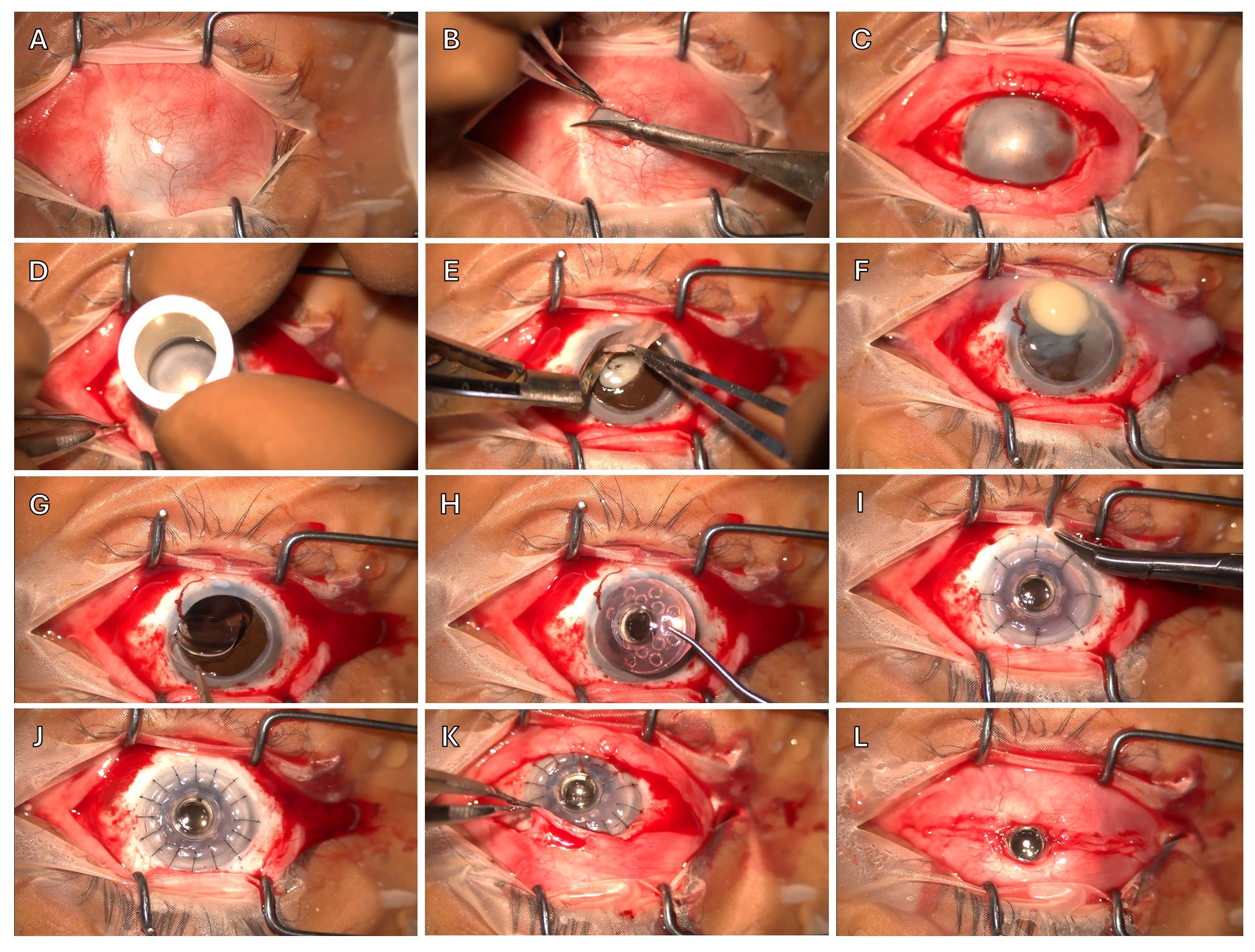
The procedure is usually performed in two stages, spaced 3 months apart. In the first stage, the dermal pannus is removed to reveal the de-epithelialized ocular surface. A 30×30-mm labial mucosal graft is harvested from the lower lip and secured over the ocular surface with four anchoring sutures, which are passed through each rectus muscle. In the second stage, the mucosal graft is lifted as a flap based on the inferior fornix. The LVP KPro is then assembled using a suitably-sized donor cornea. The recipient cornea is trephined and excised, followed by a superior sector iridectomy to reduce the risk of secondary angle closure in at least one quadrant. The eye is made aphakic by removing the crystalline or IOL, and an open-sky anterior vitrectomy is performed if the posterior capsule is breached. The LVP KPro is then sutured into place using interrupted 10-0 or 9-0 nylon sutures. The mucosal flap is repositioned and sutured with continuous interlocking 6-0 polyglactin sutures. Finally, a central cruciate opening is created in the mucosa covering the optical cylinder, with the edges tucked under the LVP KPro’s front plate. If a conjunctival flap is being used, then the procedure is single staged and the conjunctiva is closed around and under the optical stem with 7-0 polyglactin sutures. (Figure).
During the postoperative period, all patients usually have a detailed ophthalmic examination at each follow-up visit. Typically, postoperative visits are scheduled for the first day, at 4-6 weeks, and 2-3 times monthly thereafter. Postsurgery medications included topical prednisolone acetate 1% in tapering doses and moxifloxacin 0.5% eye drops four times daily. The optic disc is assessed at each visit, with visual fields evaluated every 6 months.
Outcomes
The largest series on the LVP KPro included 58 eyes of 56 patients, with 52 patients having Stevens-Johnson syndrome (SJS) as the underlying cause, three patients with a history of chemical burns, and one patient with ocular cicatricial pemphigoid (OCP).9 Among these, two patients underwent LVP KPro implantation twice in the same eye, and in two additional cases, the LVP KPro was used to replace an extruding modified OOKP (MOOKP) device. All treated eyes exhibited complete dryness with surface keratinization, and there were no significant baseline differences between pediatric and adult patients. The average postoperative follow-up was 2.5 years, with a median of 28 months. This study underscored the potential of LVP KPro as an effective treatment for patients with severe ocular surface disease, while also highlighting the necessity for vigilant postoperative management to address complications.
At the final follow-up, 81% of the implanted LVP KPros were retained without spontaneous extrusion or the need for surgical removal. Kaplan-Meier analysis indicated cumulative survival probabilities of 90.8% at 1 year, 80% at 2 years, and 76.6% at 3 years and beyond. Although pediatric patients showed better survival rates (90.9% at 5 years) compared to adults (72.3% at 5 years), this difference was not statistically significant. In terms of functional outcomes, 77.5% of eyes showed an improvement of more than two lines in BCVA from baseline at the final follow-up. The cumulative probability of maintaining 20/400 vision or better was 61.5% at 1 year, 40% at 2 years, and 37.6% at 3 years and beyond. No significant differences in functional survival were observed between children and adults at the 5-year follow-up. The median BCVA improved significantly from a baseline LogMAR value of 4 (light perception) to 1 (20/200) on the first postoperative day, with further improvements noted over time.
The most common complication observed was retroprosthetic membrane formation, requiring laser membranotomy in 43% of cases, with some necessitating surgical intervention. Progressive glaucoma was diagnosed in 25.8% of eyes, with most cases managed medically. Anatomical failure occurred in 19% of eyes, with issues such as spontaneous extrusion, pericylinder leaks leading to endophthalmitis, and the need for additional surgeries, including LVP KPro explantation and vitrectomy. Mucosal complications were observed in 19% of eyes, with some requiring regrafting or mucosal trimming.
Discussion
The LVP KPro, is a novel adaptation of the Boston type 1 KPro, that is useful in restoring vision in eyes with severe, and blinding keratopathy due to conditions such as SJS, OCP, and chemical burns. These patients were ineligible for other forms of corneal transplantation, stem cell-based therapies, or the conventional Boston type 1 keratoprosthesis implantation, highlighting the need for alternative therapeutic approaches. The retention of the LVP KPro in the majority of cases, without spontaneous extrusion or the need for surgical removal, marks a substantial advancement in the treatment of end-stage corneal diseases, particularly in cases where standard options have proven inadequate.9
When comparing the outcomes of the LVP KPro to other established keratoprosthesis devices, such as the Boston type 2 keratoprosthesis and MOOKP, the LVP KPro showed superior anatomical retention compared to the Boston type 2 but did not reach the longevity observed with MOOKP. For instance, the study referenced long-term data from Falcinelli et al, which reported a retention probability of over 90% for MOOKP at 8 years, with this figure remaining above 80% at 18 years.11 In contrast, the Boston type 2 keratoprosthesis exhibited lower retention rates, with Lee et al noting a keratoprosthesis replacement rate of 45.8% after an average follow-up of 3 years, predominantly due to corneal melting.7 These comparisons underscore the competitive performance of the LVP KPro, particularly when considering the complex cases it addresses. Functionally, while there was a noted decline in median visual acuity over time in eyes implanted with the LVP KPro, this outcome should be contextualized within the severe baseline visual impairment of the patients involved. Despite this decline, the LVP KPro still facilitated significant improvements in visual acuity for a considerable period postoperatively, suggesting that with increased surgical experience and postoperative management, functional outcomes could be further enhanced.
Serious postoperative complications occur more frequently in keratoprosthesis procedures than in other optical corneal surgeries. The LVP KPro allows for a relatively straightforward management of posterior segment complications, as retina surgeons can comfortably perform procedures such as intravitreal drug injections and sutureless 23- or 25-G vitrectomy through the mucosal graft. Furthermore, the ability to instill eye drops in the inferior fornix — a feature not possible with the OOKP or Boston type 2 keratoprosthesis — provides additional therapeutic advantages in managing intraocular inflammation and glaucoma in LVP KPro eyes. Mucosal complications, particularly in post-SJS eyes, were significantly reduced in the LVP KPro cohort compared to previous OOKP series, which can be as high as 63.3%, possibly due to the bulkiness of the bony lamina and subclinical changes in the oral mucosa associated with the disease.12,13 The ability to easily exchange the LVP KPro in cases of complications, such as extruding OOKP laminas, further emphasizes the device’s practical advantages over OOKP, where such replacements are exceedingly challenging.
Conclusion
The adaptation of the Boston type 1 keratoprosthesis design by Indian manufacturers, in collaboration with Massachusetts Eye and Ear in Boston, has allowed for the development of a low-cost version of the device, with slight modifications that retained the core advantages of the Boston KPro design. Its relative ease of implantation, coupled with improved postoperative management options, positions the LVP KPro as a compelling alternative to OOKP, particularly in cases where OOKP implantation is contraindicated or challenging, such as in children, edentulous individuals, and patients at high risk of mucosal complications. CP
References
1. Flaxman SR, Bourne RRA, Resnikoff S, et al; Vision Loss Expert Group of the Global Burden of Disease Study. Global causes of blindness and distance vision impairment 1990-2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221-e1234.
2. Gain P, Jullienne R, He Z, et al. Global survey of corneal transplantation and eye banking. JAMA Ophthalmol. 2016;134(2):167-173.
3. Sharma S, Donthineni PR, Iyer G, Chodosh J, de la Paz MF, Maskati Q, Srinivasan B, Agarwal S, Basu S, Shanbhag SS. Keratoprosthesis in dry eye disease. Indian J Ophthalmol. 2023;71(4):1154-1166.
4. Dohlman CH, Harissi-Dagher M, Khan BF, Sippel K, Aquavella JV, Graney JM. Introduction to the use of the Boston keratoprosthesis. Expert Rev Ophthalmol. 2006;1(1):41-48.
5. Zerbe BL, Belin MW, Ciolino JB; Boston Type 1 Keratoprosthesis Study Group. Results from the multicenter Boston type 1 keratoprosthesis study. Ophthalmology. 2006;113(10):1779-1184.
6. Aldave AJ, Sangwan VS, Basu S, et al. International results with the Boston type I keratoprosthesis. Ophthalmology. 2012;119(8):1530-1538.
7. Lee R, Khoueir Z, Tsikata E, Chodosh J, Dohlman CH, Chen TC. Long-term visual outcomes and complications of Boston keratoprosthesis type II implantation. Ophthalmology. 2017;124(1):27-35.
8. Michael R, Charoenrook V, de la Paz MF, Hitzl W, Temprano J, Barraquer RI. Long-term functional and anatomical results of osteo- and osteoodonto-keratoprosthesis. Graefes Arch Clin Exp Ophthalmol. 2008;246(8):1133-1137.
9. Basu S, Nagpal R, Serna-Ojeda JC, Bhalekar S, Bagga B, Sangwan V. LVP keratoprosthesis: anatomical and functional outcomes in bilateral end-stage corneal blindness. Br J Ophthalmol. 2018 Jun 11:bjophthalmol-2017-311649.
10. Basu S, Sureka S, Shukla R, Sangwan V. Boston type 1 based keratoprosthesis (Auro KPro) and its modification (LVP KPro) in chronic Stevens Johnson syndrome. BMJ Case Rep. 2014;2014:bcr2013202756.
11. Falcinelli G, Falsini B, Taloni M, Colliardo P, Falcinelli G. Modified osteo-odonto-keratoprosthesis for treatment of corneal blindness: long-term anatomical and functional outcomes in 181 cases. Arch Ophthalmol. 2005;123(10):1319-1329.
12. Basu S, Pillai VS, Sangwan VS. Mucosal complications of modified osteo-odonto keratoprosthesis in chronic Stevens-Johnson syndrome. Am J Ophthalmol. 2013;156(5):867-873.
13. Tan A, Tan DT, Tan XW, Mehta JS. Osteo-odonto keratoprosthesis: systematic review of surgical outcomes and complication rates. Ocul Surf. 2012;10(1):15-25.
